
More Information
Submitted: March 19, 2026 | Accepted: March 31, 2026 | Published: April 01,, 2026
Citation: Ladegard KM, et al. Bringing Mental Health Treatment to Youth: Integrated School-Based Health Centers in Urban Schools. Clin J Nurs Care Pract. 2026; 10(1): 008-015. Available from:
https://dx.doi.org/10.29328/journal.cjncp.1001062.
DOI: 10.29328/journal.cjncp.1001062
Copyright License: © 2026 Ladegard KM, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: School-based mental health treatment; Youth mental health; Academic performance; Suicide

Bringing Mental Health Treatment to Youth: Integrated School-Based Health Centers in Urban Schools
Kristie M Ladegard1*, Christian C Thurstone2, Angela Keniston3, Ryan Loh4, Sonja O'Leary5 and Steven Solomon6
1University of Colorado, Director of Psychiatry School Based Clinics Denver Health Hospital and Authority 777 Bannock Street, Denver, CO 80204, USA
2Division of Substance Dependence University of Colorado Denver, Medical Director of Behavioral Health Denver Health and Hospital Authority 723 Delaware Street, Denver, CO 80204, USA
3Division of Hospital Medicine University of Colorado Leprino Office Building 12401 E. 17th Avenue, Mail Stop F782 Aurora, CO 80045, USA
4Denver Health 77 W. 5th Ave. MC7993 Denver CO 80204, USA
5Department of Pediatrics University of Colorado School of Medicine, Chair Ambulatory Pediatrics and Community Programs at Denver Health 601 Broadway MC 7779 Denver CO 80204, USA
6Health One Presbyterian Saint Luke 1830 N. Franklin Street Denver CO 80218, USA
*Corresponding author: Kristie M Ladegard, University of Colorado, Director of Psychiatry School Based Clinics Denver Health Hospital and Authority, 777 Bannock Street, Denver, CO 80204, USA, Email: [email protected]
Background: The youth health problems are very prevalent in the United States. Approximately one in five children and adolescents experience mental health problems, yet many have limited access to appropriate treatment, contributing to increased suicidal risks and school failure. School-based health centers (SBHCs) offer a promising avenue to deliver care where students spend most of their time.
Aim: This study examined associations between SBHC-delivered mental health services and changes in students’ mental health symptoms, functioning, and school-related outcomes in a large urban district.
Methods: Mental health symptoms and functioning were assessed using the Ohio Youth Problem Functioning and Satisfaction Scales at baseline and approximately 3 and 6 months after initiation of school-based mental health treatment. Linked educational records provided grade point average (GPA), attendance, and behavioral incident data for 1,238 students receiving services between 2010 and 2019. One-way repeated measures analysis of variance was used to examine within-student changes over time, including analyses stratified by baseline symptom severity and functional impairment.
Results: School-based mental health treatment was associated with reduced problem severity, particularly among students with the highest baseline symptom burden, including self-harm, thoughts of death, and sadness/depression, and with improved functioning in those with severe initial impairment. GPA increased modestly, and behavioral incidents decreased by about half in the year following treatment compared with the prior year, while attendance showed smaller improvements. Youth and parent reports demonstrated similar patterns of change.
Conclusion: In this urban SBHC system, participation in school-based mental health services was associated with improvements in student mental health and favorable changes in school-related behaviors and performance. Although causal inference is limited by the observational design, these results add to evidence that SBHC mental health services may play an important role in supporting youth functioning, behavior, and academic outcomes.
Youth mental health problems are highly prevalent and often undertreated in the United States, resulting in substantial personal, educational, and societal burdens. More than 20% of children and adolescents experience mental health concerns [1], and inadequate access to effective treatment increases risk for suicidal behaviors and school failure. Suicide is the second leading cause of death among youth ages 10–24 [2] with recent surveillance data indicating that over one in ten high school students report a suicide attempt and more than one in five seriously consider suicide [3]. These mental health challenges also undermine educational attainment; students with mental health disorders have higher dropout rates than peers with other disabilities [4], and leaving school early markedly increases the likelihood of unemployment in adulthood. Together, these data underscore a persistent, high‑stakes need for accessible, effective youth mental health services.
Despite this need, many young people face structural and practical barriers to community mental health care, including transportation difficulties, limited insurance coverage, stigma, and lack of child‑trained providers. Less than half of youth with a mental health condition receive any treatment in a given year [5], and those who do often encounter fragmented, time‑limited services that are insufficient to achieve sustained symptom improvement [6,7]. These barriers disproportionately affect youth in low‑income and racially and ethnically minoritized communities, contributing to inequities in both mental health and educational outcomes. Identifying service models that reduce access barriers and can be embedded in youths’ everyday environments is, therefore, a critical public health and education priority.
Schools occupy a central position in efforts to address this gap because they have near‑universal contact with children and adolescents and a mandate to promote both safety and learning. Over 90% of U.S. youth spend most weekdays in school [8], making schools a natural venue for identifying mental health concerns early, engaging families, and coordinating supports. Within this context, school‑based health centers (SBHCs) have emerged as an important strategy for delivering integrated medical and behavioral health services directly on or near school campuses. A growing proportion of SBHCs now provide mental health care, often through multidisciplinary teams that include behavioral health clinicians alongside primary care providers. By locating services where students already are, SBHCs can reduce logistical barriers, normalize help‑seeking, and facilitate sustained engagement in treatment.
A growing body of research suggests that SBHC mental health services may improve both psychiatric symptoms and school‑related behaviors. One study demonstrated that an increase in the availability of mental health services provided by 14 public schools with SBHCs from 2013 to 2015 was associated with significant reductions in the likelihood of depressive episodes and suicide risk among adolescents [9]. Other studies have linked SBHC utilization to improved academic outcomes, including higher grade point averages and better college preparation, as well as higher graduation and grade promotion rates [10,11]. These benefits may arise in part because SBHC providers can address long‑term health conditions such as mental health challenges, which are known to lower academic performance [12-14]. According to the U.S. Centers for Disease Control and Prevention (CDC), academic performance and health are bidirectionally linked: learning improves health, but health is also a prerequisite to effective learning [15]. While physical health impacts academic performance, poor childhood mental health is also negatively correlated with educational attainment [12,13]. Data showing that school‑based mental health services reduce the likelihood of behaviors like skipping school or being late suggest that mental health services provided through SBHCs may improve academic performance through constructive changes in behavior [15-18]. Students with lower levels of academic performance not only use SBHCs for mental health services more than those with higher performance but also undergo sharper improvements in their academic performance after initiating this care [19-21].
Despite this promising literature, important gaps remain. Many prior evaluations of SBHC mental health services have relied on cross‑sectional or short‑term designs, limiting the ability to describe trajectories of change in symptoms and functioning over time [9,11,13]. Few studies have combined repeated, standardized mental health measures with objective academic data such as GPA, attendance, and behavioral incidents within a large, diverse urban school district [10,11,16,21]. There is also limited evidence regarding whether students with the most severe baseline problems derive greater benefit from SBHC mental health services than those with milder concerns, an issue with direct implications for targeting and resource allocation. Addressing these gaps is essential to inform local and state decisions about investing in and scaling school‑based mental health programs.
The current study was designed to address these needs by examining the impact of mental health services delivered through Denver School‑Based Clinics (DSBCs), a network of SBHCs serving predominantly inner‑city youth in Denver, Colorado. DSBCs operate within a large, socioeconomically and racially diverse public school district, where nearly half of students are economically disadvantaged, and a substantial majority identify as youth of color [22]. These clinics provide comprehensive mental health care, including psychotherapy, medication management, family interventions, and crisis services, embedded in students’ school environments. Leveraging repeated assessments from the Ohio Youth Problem Functioning and Satisfaction Scales (Ohio Scales) alongside linked educational records, this study follows a large cohort of students receiving DSBC mental health services over time.
Based on prior work, the primary hypothesis is that participation in SBHC mental health services will be associated with reductions in symptom severity and improvements in functioning on the Ohio Scales, as well as better academic performance reflected in higher GPA, improved attendance, and fewer behavioral incidents. A secondary hypothesis is that students with greater baseline symptom burden or functional impairment will demonstrate larger gains than their peers with less severe initial presentations. By integrating standardized mental health measures with academic outcomes in a real‑world urban SBHC system, this research aims to clarify the potential impact of school‑based mental health services on student mental health and school performance and to generate evidence relevant to other districts considering similar models of care.
This observational cohort study examined changes in mental health symptoms, functioning, and school-related outcomes among students receiving mental health services in Denver School-Based Clinics (DSBCs) over nine years, using repeated standardized assessments and linked educational records. These methodological details are provided to help readers judge the applicability of these findings to their own SBHC and school contexts.
Setting
DSBCs are integrated school-based health centers embedded in 11 public schools in Denver, Colorado, serving a socioeconomically and racially diverse urban student population. The participating schools included middle schools, high schools, combined 6th–12th grade schools, a school for pregnant and parenting teens and their children, and an arts academy spanning kindergarten through 12th grade. As part of a larger district in which nearly half of the students are economically disadvantaged, and the majority identify as youth of color, DSBCs provide on‑site comprehensive health services with an emphasis on mental health care.
Mental health services in DSBCs are delivered by a multidisciplinary team that includes Licensed Clinical Social Workers (LCSWs) and Child/Adolescent Psychiatrists. School-based mental health services were first established in the 11 original SBHCs in 2010, and the network subsequently expanded to 19 locations across Denver; however, for analytic consistency, only data from the original 11 clinics were included in this study. This focus on the initial cohort of clinics ensures a stable service model and follow‑up structure over the study period while reflecting a typical urban SBHC configuration.
Data sources
Clinical and mental health data: The primary clinical outcome data were collected using the Ohio Youth Problem Functioning and Satisfaction Scales (OYPFSS, “Ohio Scales”), a standardized set of measures designed to monitor youth mental health treatment outcomes [23]. Both youth and parents completed parallel versions of the scales, which assess four domains: problem severity, functioning, hopefulness, and satisfaction with treatment. Each domain uses Likert‑type response options, with higher problem severity scores indicating worse symptoms and higher functioning scores indicating better functioning; lower scores on the satisfaction and hopefulness scales reflect greater satisfaction and more positive expectations, respectively. Surveys were administered at baseline (initial mental health visit) and at approximately 3, 6, 9, and 12 months thereafter; for the present analyses, data were restricted to baseline, 3‑month, and 6‑month assessments because attrition at 9 and 12 months substantially reduced sample sizes at those time points. The OYPFSS has demonstrated internal consistency and test–retest reliability in prior work [24], supporting its use as an outcome measure in school-based mental health settings.
Educational records: Educational data were obtained from students’ school records and included grade point average (GPA), school attendance, and behavioral incidents. GPA was extracted for defined periods spanning the year before treatment and the year following the initiation of school-based mental health services, including six academic terms when available. Attendance data reflected days or classes missed over comparable intervals, allowing examination of changes before and after treatment initiation. Behavioral incidents were defined using school documentation of problem behaviors, including but not limited to disrupting class, walking out of class, engaging in verbal or physical altercations with other students or staff, and fighting. For each student with available records, the annual number of behavioral incidents was calculated for the year before and the year following initiation of mental health treatment.
Sample
Recruitment occurred on a rolling basis between 2010 and 2019 as part of routine DSBC clinical workflows. Eligible participants were students between the ages of 12 and 21 who were enrolled in mental health treatment at one of the 11 participating schools with SBHC sites and who completed at least a baseline OYPFSS assessment. The research project was approved by the Colorado Multiple Institutional Review Board on July 28th, 2015. These schools served a heterogeneous student population across multiple grade configurations, including middle schools, high schools, 6th–12th grade schools, a school for pregnant and parenting teens and their children, and a K–12 arts academy. Students who were enrolled in SBHC mental health services but did not complete the surveys, or whose responses could not be linked to educational records for specific analyses, were excluded from the corresponding analyses.
In total, 1,238 students were included in the final student sample, and 81 parents contributed parent-report surveys. Data collection for each youth began at the initial intake mental health visit and continued at subsequent follow‑up visits when surveys were administered. Analytic sample sizes varied by outcome: for example, n = 139 youth contributed to the 6‑month problem severity analysis, n = 133 to the 6‑month functioning analysis, 192 students had linked GPA data for pre–post comparisons, and 490 students had analyzable behavioral incident data. Youth participants under age 18 provided assent with parental consent via the school-based clinic consent process, while those aged 15–17 could access mental health care without separate parental consent under Colorado law; however, a parent or guardian was still required to complete the general school-based clinic consent form for the youth to be seen. Parents of students receiving mental health care at DSBCs were invited to complete parallel OYPFSS forms when present and willing to participate.
Statistical analyses
In this study, means and standard deviations (SDs) were generated for continuous variables when normally distributed, medians and interquartile ranges (IQRs) when not, and frequencies for categorical variables. Descriptive statistics were computed, initially examining demographics for students who completed assessments at each time-point.
82 students completed the surveys at 9 months, and 32 students completed them 12 months after behavioral health services interventions were initiated. These time-points were therefore excluded from the statistical analysis, which we limited to an assessment of data from baseline, three months, and six months. One-way repeated measures analysis of variance (ANOVA) was used to investigate changes in youth scores in all four parts of the OYPFSS across the three time points. One-way repeated measures ANOVAs were employed to examine potential changes in GPA, over three years, including six terms, school attendance, and behavioral incidences before and after behavioral health services were initiated. Bonferroni's correction for multiple comparisons was applied, with p < 0.007 considered statistically significant. Here, the use of p < 0.007 is the result of correcting for multiple comparisons, whereby a more conservative cut-off for statistical significance was used to avoid a Type I error. Effect sizes for significant results are reported throughout using Cohen’s d. All statistical analyses for this study were performed using SAS Enterprise Guide 7.1 (SAS Institute, Inc., Cary, North Carolina).
Table 1 summarizes baseline characteristics of the 1,238 students and 81 parents included in the study sample. The average age of youth participants was 14 years, with more students identifying as male than female and approximately half self‑identifying as Hispanic, reflecting the broader demographics of the district. Missing data for gender and race were common, in part because these items were located at the top of the Ohio Scales form and offered limited response options, a limitation that is addressed further in the Discussion.
| Table 1: Baseline demographic characteristics for all participants. | |
| Variables | N = 1,238 |
| Age in years – mean (SD) | 14 + 2 |
| Ethnicity | |
| Hispanic/Latino – n (%) | 615 (50) |
| Not Hispanic/Latino – n (%) | 623 (50) |
| Race | |
| African American – n (%) | 147 (12) |
| Caucasian – n (%) | 193 (16) |
| Other – n (%) | 42 (3) |
| Missing – n (%) | 856 (69) |
| Gender | |
| Female – n (%) | 365 (29) |
| Male – n (%) | 525 (42) |
| Missing – n (%) | 348 (28) |
Completion of follow‑up assessments declined over time, with most students not completing surveys at 9 and 12 months, leading analyses to focus on baseline, 3‑month, and 6‑month data. Despite this attrition, comparisons between completers and non‑completers showed no statistically significant differences in age, race, ethnicity, or gender at either 3 or 6 months, suggesting limited systematic bias due to loss to follow‑up. For example, mean age and the proportion of Hispanic/Latino students were similar across groups at both time points, and the proportion of non‑Caucasian students and females among completers did not differ significantly from non‑completers (Table 2).
| Table 2: Comparison of youth who did and did not complete follow-up by age, ethnicity, race, and sex. | ||||||
| Variables | Completed at 3 months N = 275 |
Not completed at 3 months N = 963 |
p -value | Completed at 6 months N = 208 |
Not completed at 6 months N = 1,030 |
p -value |
| Age – years (SD) | 14.3 + 1.8 | 14.4 +1.9 | 0.4201 | 14.2 + 1.7 | 14.4 + 1.9 | 0.2602 |
| Ethnicity %Hispanic/Latino | 146 (53) | 469 (49) | 0.1992 | 106 (51) | 509 (49) | 0.6846 |
| Race - % non-Caucasian | 40 (15) | 149 (15) | 0.0746 | 37 (18) | 152 (15) | 0.0703 |
| Sex - % female | 151 (55) | 374 (39) | 0.1235 | 94 (45) | 431 (42) | 0.0734 |
| Sex - % male | 88 (32) | 277 (29) | 49 (24) | 316 (87) | ||
During the 6 months of school‑based mental health treatment, youth reported significant improvements in core mental health outcomes as measured by the Ohio Scales. Across all participants with available data, problem severity scores decreased (n = 139, p < 0.0001, d = 0.48), functioning scores increased (n = 133, p = 0.01, d = 0.11), and satisfaction with treatment improved (n = 116, p = 0.005, d = 0.40), while parent‑rated hopefulness remained stable (n = 124, p = 0.10; Figure 1). Item‑level and subgroup analyses showed that high‑risk behaviors such as self‑harm, talking or thinking about death, and feeling sad or depressed declined over time, with the largest relative reduction observed for talking or thinking about death (Table 3).
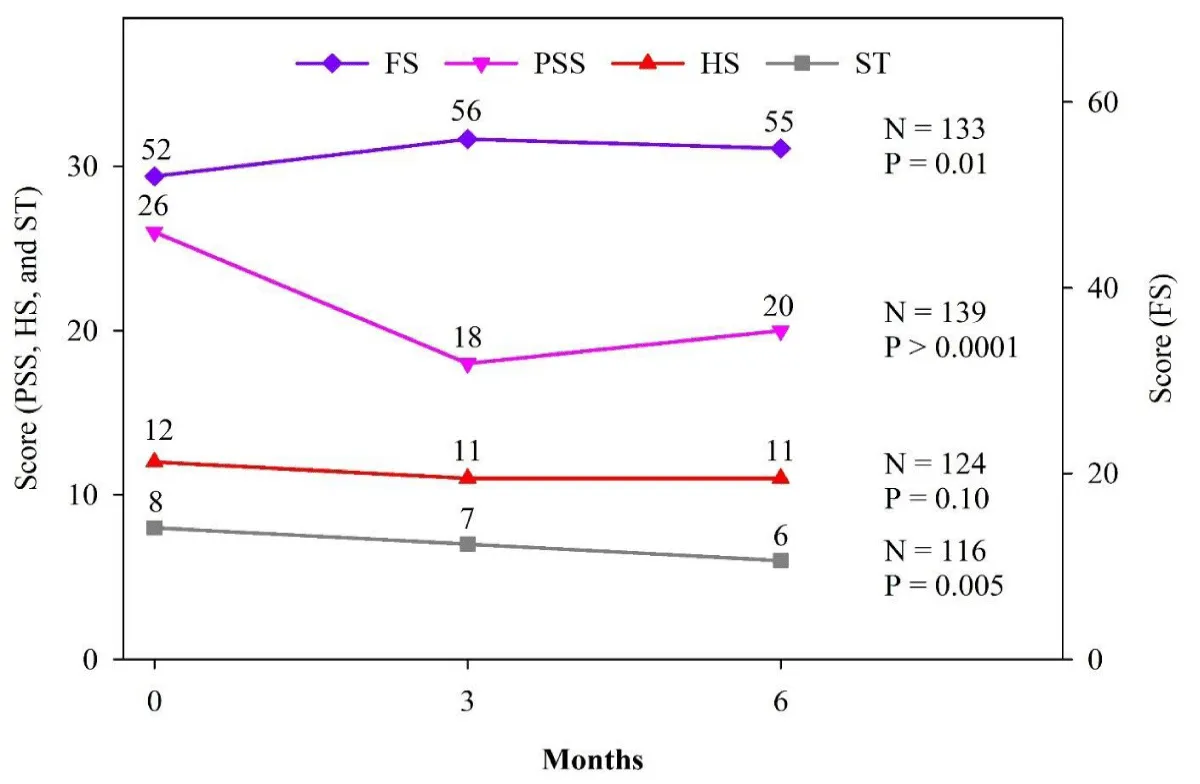
Figure 1: Student scores on the Ohio Youth Problem Severity Scale (PSS), Functioning Scale (FS), and Satisfaction with Treatment (ST).
| Table 3: Mental health treatment and changes in high-risk behavioursby baseline problem severity. | |||||
| Problem severity and functioning score | Baseline N (%) |
3 Months N (%) |
6 Months N (%) |
ARR (%) | RRR (%) |
| Problem Severity Scale Questions | |||||
| Using drugs or alcohol | 8 (16) | 8 (16) | 8 (16) | ||
| Skipping school/classes | 11 (22) | 11 (22) | 15 (30) | ||
| Hurting self | 16 (32) | 8 (16) | 6 (12) | 20 | 62.5 |
| Talking/thinking about death | 26 (52) | 14 (27) | 12 (24) | 28 | 54 |
| Feeling anxious or fearful | 32 (64) | 24 (48) | 27 (54) | ||
| Feeling sad or depressed | 32 (64) | 25 (50) | 26 (52) | 12 | 23 |
| Functioning Scale Questions | |||||
| Attending school and getting passing grades at school | 8 (20) | 11 (27.5) | 10 (25) | ||
| ARR = Absolute Risk Reduction, RRR = Relative Risk Reduction. | |||||
When outcomes were stratified by baseline severity and impairment, youth with the highest initial problem severity and functional impairment experienced the greatest gains. Among those with many problems at baseline, problem severity scores decreased by 11 points (n = 33, p < 0.0001, d = 1.29), whereas changes were smaller and not statistically significant for youth with some or no baseline problems (Figure 2). Similarly, functioning scores improved most in youth with severe initial impairment (mean increase of 12 points, n = 20, p = 0.0015, d = 0.83), with smaller improvements among those with some impairment and minimal change among those without baseline impairment (Figure 3).
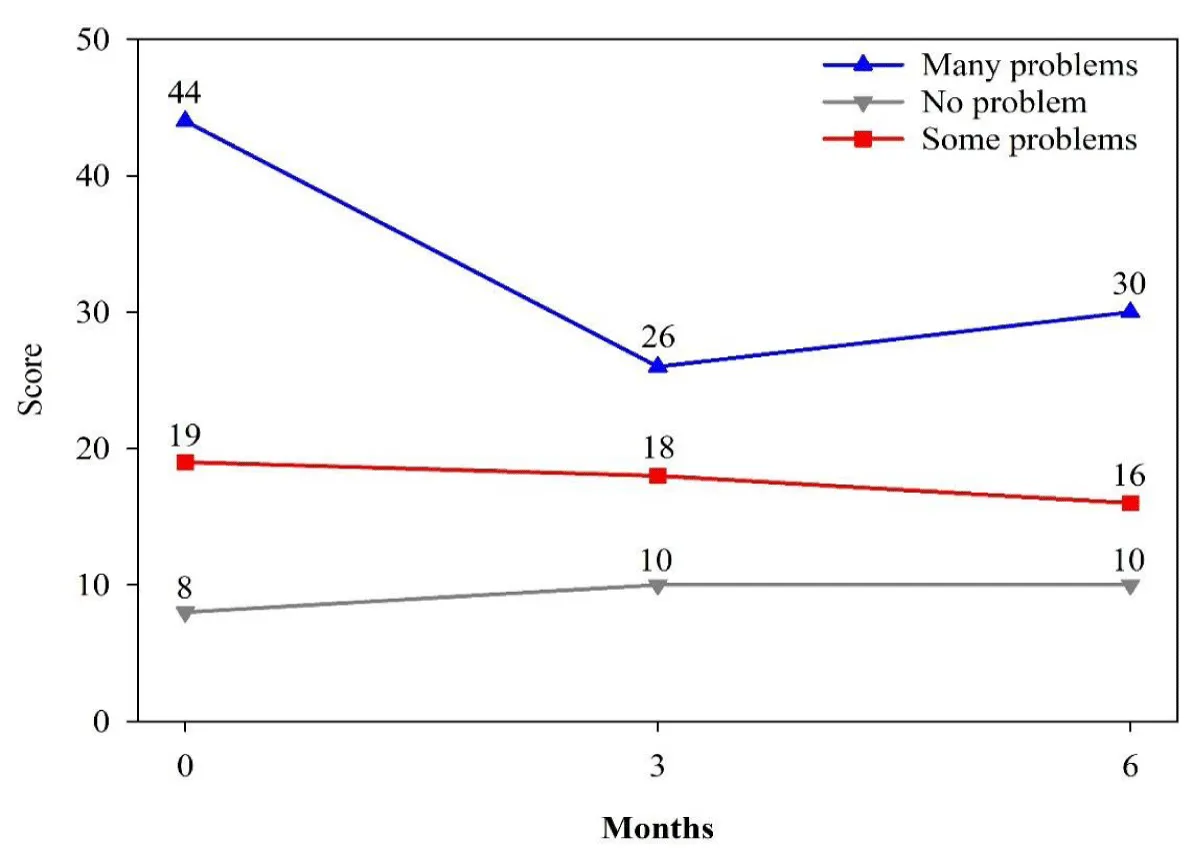
Figure 2: Youth Problem Severity Scale Score over Time by Level of Severity at Baseline, N = 139.
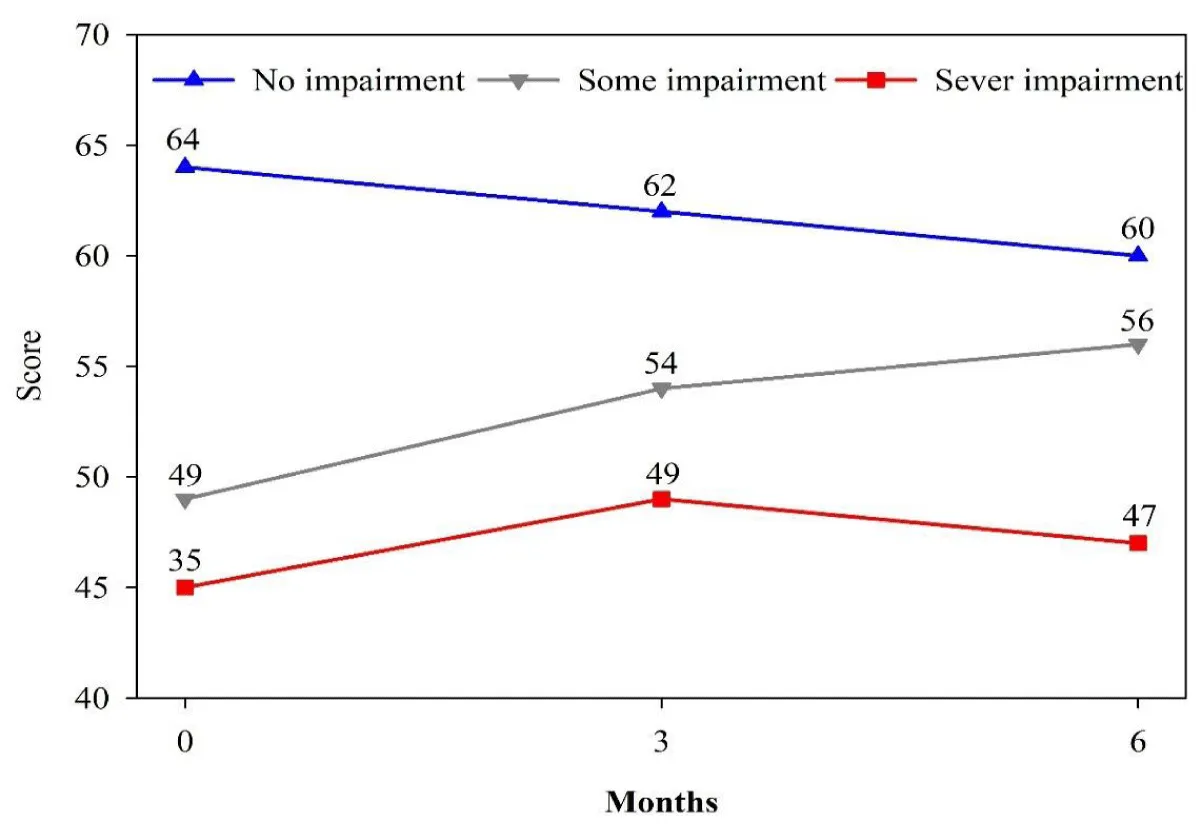
Figure 3: Youth Functioning Scale Score over Time by Level of Severity at Baseline, N = 133.
School‑based mental health treatment was also associated with improvements in academic‑related outcomes. Among the 192 students with analyzable GPA data, mean GPA increased from 2.4 in the year before treatment to 2.6 in the year following treatment (p = 0.0007, d = 0.25; Table 4). For the 490 students with behavioral incident data, the average number of documented incidents per year—such as classroom disruption, walking out of class, verbal or physical altercations, and fighting—declined from 1.2 before treatment to 0.6 after treatment (p < 0.0001, d = 0.36; Table 4). Attendance showed more modest changes, with small improvements consistent with the overall pattern of behavioral gains.
| Table 4: Participants’ academic outcomes. | |||||||
| Attendance and behavioral outcomes | Year Before Treatment | Year During Treatment | p -value | ||||
| Attendance - # missed classes per year N = 475 | 67 + 44 | 64 + 34 | 0.0192 | ||||
| Behavioral incidents - # per year N = 490 | 1.2 + 1.8 | 0.6 + 0.7 | <.0001 | ||||
| Academic outcomes | One Year Pre-treatment Term 1 | One Year Pre-treatment Term 2 | Current School Year Term 1 | Current School Year Term 2 | One Year Post Treatment Term 1 | One Year Post Treatment Term 2 | p -value |
| Grade point average – mean by semester+SDN = 192 | 2.4 + 1.0 | 2.4 + 1.0 | 2.5 + 1.0 | 2.3 + 1.0 | 2.6 + 1.0 | 2.6 + 1.0 | <.0001 |
Parent reports generally paralleled youth self‑reports, providing convergent evidence for treatment‑associated improvements. When parents completed the Ohio Scales, their ratings indicated decreases in their children’s problem severity and improvements in functioning over the 6 months, with patterns similar to those observed in youth responses (Figure 4). Taken together, these findings suggest that mental health services delivered in the original 11 Denver school‑based clinics were associated with reductions in problem severity, enhanced functioning, and improvements in school‑related behaviors, including GPA and behavioral incidents.
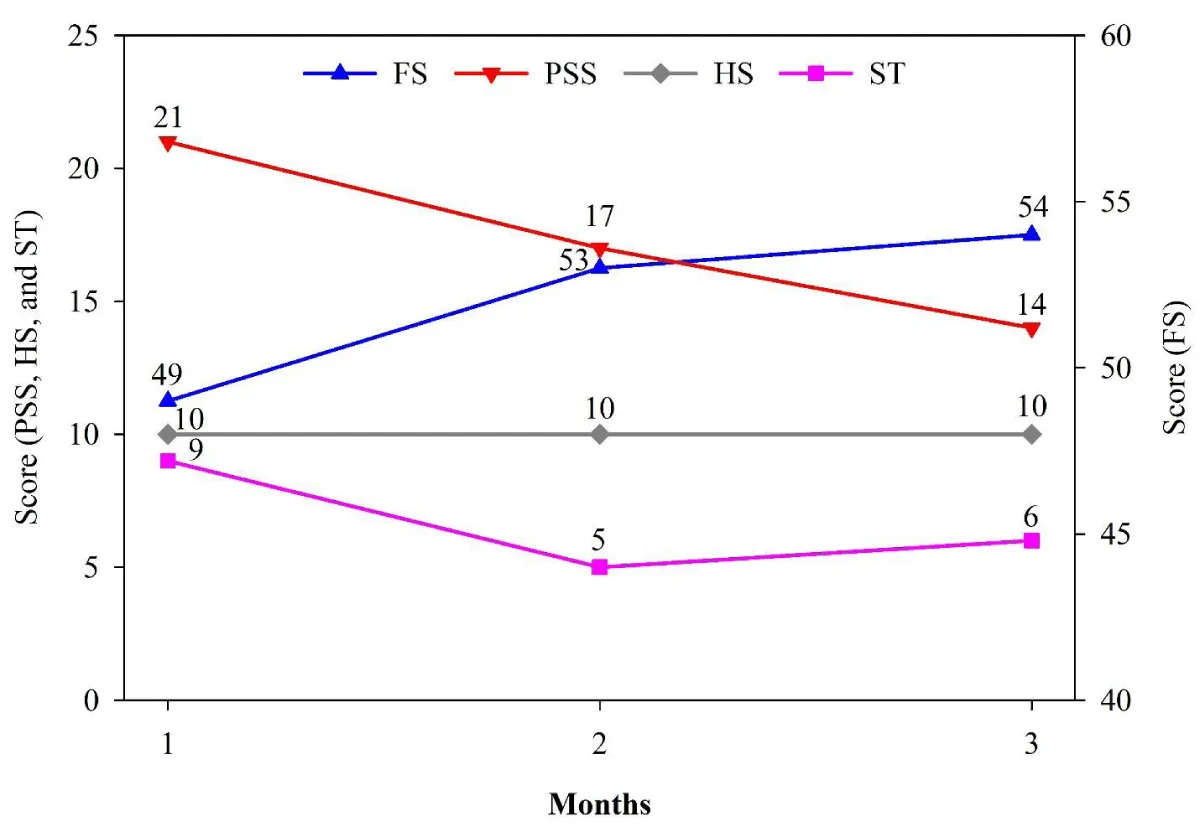
Figure 4: Parent results on Ohio Youth Problem Severity (PSS), Functioning (FS), Satisfaction with Treatment (ST), and Hopefulness Scales (HS).
SBHCs play a pivotal role in providing accessible physical and mental health services, with growing evidence underscoring the importance of mental health as a determinant of both student well-being and educational outcomes [24]. In this study of more than 1,200 students receiving care in Denver School-Based Clinics, school-based mental health treatment was associated with decreased problem severity, particularly among youth with the highest baseline symptom burden, including self‑harm, thoughts of death, and sadness/depression. Functioning improved over six months of treatment, with the largest gains observed in students who began with severe impairments, while parent and youth ratings showed similar patterns of change, adding confidence that these improvements reflect meaningful clinical benefit. Academic‑related outcomes also improved: GPA increased modestly, behavioral incidents were cut roughly in half, and attendance showed small gains over the observation period. These findings are consistent with prior work demonstrating that SBHC mental health services are associated with reductions in depression and suicidal ideation [25,26], as well as studies showing that SBHC use is linked to higher GPA and reduced absenteeism [27,28]. What is relatively new here is the combination of repeated, standardized symptom and functioning measures with objective academic data across multiple terms in a large urban district, along with stratified analyses indicating that students with the greatest initial needs experienced the largest improvements.
The present results have several implications for Denver’s SBHC system and for other districts considering expansion of school-based mental health services. For Denver, the observed reductions in symptom severity and improvements in functioning and school-related behaviors provide empirical support for continued and potentially expanded investment in integrated mental health services within SBHCs, particularly for students presenting with high levels of distress or functional impairment. For other districts and state systems, these findings suggest that school-based mental health programs embedded in SBHCs may contribute to both mental health and educational goals, reinforcing the case for funding models that prioritize services in schools serving socioeconomically and racially marginalized youth. By documenting associations with GPA and behavioral incidents, the study also offers data that can be used in arguments for equity‑focused placement of SBHCs and closer alignment of mental health initiatives with school improvement plans, without yet prescribing a specific policy framework.
At the same time, several limitations should be considered when interpreting these findings. The study used an observational design without a randomized control group, so causal inferences about the impact of SBHC mental health services are necessarily limited, and some improvements may reflect regression to the mean or concurrent services outside SBHCs. Outcomes relied in part on self‑report, which is vulnerable to expectancy or social desirability biases; the mental health interventions were not manualized and could vary in intensity and content across clinicians and sites; and detailed data on specific treatment modalities were not available. High attrition beyond six months constrained examination of longer‑term trajectories, and the use of a form with only two gender options, combined with the single‑district, Denver‑only setting, may limit generalizability to non‑binary youth and to other regions or SBHC systems. In addition, reduced sample sizes in some analyses—for example, the 6‑month problem severity cohort and the severely impaired functioning subgroup—may limit the precision of these estimates and further constrain the generalizability of subgroup findings, and thus should be interpreted with caution.
This study also has notable strengths that support the relevance of its findings to school-based mental health practice. It draws on a large, diverse urban sample across multiple school types, uses a standardized, psychometrically supported outcome measure (the Ohio Scales) administered repeatedly over several time points, and links these data to objective academic records including GPA, attendance, and behavioral incidents. The stratified analyses by baseline severity and impairment illustrate that students with the highest needs appear to benefit most, a pattern that is highly relevant for resource targeting, and the convergence between youth and parent ratings strengthens confidence in the observed direction and magnitude of change. Together, these features position the study as a useful contribution to the emerging evidence base on the potential impact of school-based mental health services delivered through SBHCs.
School-based health centers in Denver were associated with meaningful improvements in students’ mental health, including reduced problem severity—particularly for youth reporting self‑harm, thoughts of death, and sadness/depression—and improved functioning over six months of treatment. Academic outcomes also moved in a favorable direction, with modest gains in GPA and notable reductions in behavioral incidents, suggesting potential spillover benefits of mental health care for school performance and behavior. Because this was an observational study without a randomized control group, these findings should be interpreted as evidence of association rather than proof of causation, and concurrent services or unmeasured factors may have contributed to observed changes. Future research using more rigorous designs, longer follow‑up, and richer characterization of intervention components is needed to clarify the causal impact of SBHC mental health services and to guide optimization and scaling of these models in diverse school settings.
- Merikangas KR, He JP, Burstein M, Swendsen J, Avenevoli S, Case B, et al. Service utilization for lifetime mental disorders in U.S. adolescents: results of the national comorbidity survey-adolescent supplement (NCS-A). J Am Acad Child Adolesc Psychiatry. 2011;50:32-45. Available from: https://doi.org/10.1016/j.jaac.2010.10.006
- Hua LL, Lee J, Rahmandar MH, Sigel EJ. Suicide and suicide risk in adolescents. Pediatrics. 2024;153(1):e2023064800. Available from: https://doi.org/10.1542/peds.2023-064800
- Kann L, McManus T, Harris WA, Shanklin SL, Flint KH, Queen B, et al. Youth risk behavior surveillance—United States, 2017. MMWR Surveill Summ. 2018;67(8):1-114. Available from: https://doi.org/10.15585/mmwr.ss6708a1
- Ruch DA, Sheftall AH, Schlagbaum P, Rausch J, Campo JV, Bridge JA. Trends in suicide among youth aged 10 to 19 years in the United States, 1975 to 2016. JAMA Netw Open. 2019;2(5):e193886. Available from: https://doi.org/10.1001/jamanetworkopen.2019.3886
- The Commonwealth Fund. Understanding the U.S. behavioral health workforce shortage. 2023 May 18. Available from: https://www.commonwealthfund.org/publications/explainer/2023/may/understanding-us-behavioral-health-workforce-shortage
- Mew EJ, Blas V, Winschel J, Hunt L, Soliai-Lemusu SI, Johansson A, et al. There are still broken or fragmented systems: qualitative assessment of needs to strengthen adolescent mental health services in American Samoa. Int J Ment Health Nurs. 2024;33(1):85-92. Available from: https://doi.org/10.1111/inm.13223
- Omiyefa S. Mental healthcare disparities in low-income US populations: barriers, policy challenges, and intervention strategies. Int J Res Publ Rev. 2025;6(3):2277-2290. Available from: https://doi.org/10.55248/gengpi.6.0325.1186
- Ross SE, Flynn JI, Pate RR. What is really causing the obesity epidemic? A review of reviews in children and adults. J Sport Sci. 2015;2:1-6. Available from: https://doi.org/10.1080/02640414.2015.1093650
- Mackie P, Sim F. Improving the health of children and young people: the World Health Organization Global Schools Health initiative twenty-three years on. Public Health. 2018;159:A1-A3. Available from: https://doi.org/10.1016/j.puhe.2018.05.012
- Westbrook M, Martinez L, Mechergui S, Yeatman S. The influence of school-based health center access on high school graduation: evidence from Colorado. J Adolesc Health. 2020;67(3):447-449. Available from: https://doi.org/10.1016/j.jadohealth.2020.04.012
- Keeton V, Soleimanpour S, Brindis CD. The evidence on school-based health centers: a review. Glob Pediatr Health. 2019;6:1-12. Available from: https://doi.org/10.1177/2333794X19828745
- Grotan K, Sund ER, Bjerkeset O. Mental health, academic self-efficacy and study progress among college students—the SHOT study, Norway. Front Psychol. 2019;10:45. Available from: https://doi.org/10.3389/fpsyg.2019.00045
- Brannlund A, Strandh M, Nilsson K. Mental health and educational achievement: the link between poor mental health and upper secondary school completion and grades. J Ment Health. 2017;26(4):318-325. Available from: https://doi.org/10.1080/09638237.2017.1294739
- Michael SL, Merlo CL, Basch CE, Wentzel KR, Wechsler H. Critical connections: health and academics. J Sch Health. 2015;85(11):740-758. Available from: https://doi.org/10.1111/josh.12309
- Arenson M, Hudson PJ, Lee N, Lai B. The evidence on school-based health centers: a review. Glob Pediatr Health. 2019;6:1-10. Available from: https://doi.org/10.1177/2333794x19828745
- Paschall MJ, Bersamin M, Finan LJ, Zhang L. School-based health services and educational attainment: findings from a national longitudinal study. Prev Med. 2019;121:74-78. Available from: https://doi.org/10.1016/j.ypmed.2019.02.019
- Guzmán J, Kessler RC, Squicciarini AM, George M, Baer L, Canenguez KM, et al. Evidence for the effectiveness of a national school-based mental health program in Chile. J Am Acad Child Adolesc Psychiatry. 2015;54(10):799-807.e1. Available from: https://doi.org/10.1016/j.jaac.2015.07.005
- Gall G, Pagano ME, Desmond MS, Perrin JM, Murphy JM. Utility of psychosocial screening at a school-based health center. J Sch Health. 2000;70(7):292-298. Available from: https://doi.org/10.1111/j.1746-1561.2000.tb07254.x
- Amaral G, Geierstanger S, Soleimanpour S, Brindis C. Mental health characteristics and health-seeking behaviors of adolescent school-based health center users and nonusers. J Sch Health. 2011;81(3):138-145. Available from: https://doi.org/10.1111/j.1746-1561.2010.00572.x
- Szumilas M, Kutcher S, Leblanc JC, Langille DB. Use of school-based health centres for mental health support in Cape Breton, Nova Scotia. Can J Psychiatry. 2010;55(5):319-328. Available from: https://doi.org/10.1177/070674371005500508
- Walker SC, Kerns SEU, Lyon AR, Bruns EJ, Cosgrove TJ. Impact of school-based health center use on academic outcomes. J Adolesc Health. 2010;46(3):251-257. Available from: https://doi.org/10.1016/j.jadohealth.2009.07.002
- Denver Public Schools. About DPS. Available from: http://thecommons.dpsk12.org/domain/55
- Ohio Scales for Youth. The scales. 2023. Available from: https://sites.google.com/site/ohioscales/the-scales
- Nelson KL, Chambless K, Panicker DS, Holtz K, Hacker ME, Banks M. The school health hub: an interdisciplinary school-based mental health program to promote access, equity, student well-being, and academic progress. J Prev Health Promot. 2026;7(2):322-348. Available from: https://doi.org/10.1177/26320770251384660
- Duck AA, Carr K, Lim CS, Robinson JC. Integrating behavioral health and primary care in an inner-city high school: expanded care in a school-based clinic in Mississippi, 2018-2020. Public Health Rep. 2023;138(1 Suppl):16S-21S. Available from: https://doi.org/10.1177/00333549221128221
- Smith BM, Prichett L, Yousefzadeh N, Tschudy MM, Johnson SB, Connor KA. Emergency department visits for mental and behavioral health disorders by students enrolled in a school-based health center. Fam Syst Health. 2025;43(1):38-48. Available from: https://doi.org/10.1037/fsh0000939
- Gruber JA, Anderson-Carpenter KD, McNall M, Clark SL. Understanding the longitudinal impact of school-based health centers on student attendance. Child Youth Care Forum. 2023;52(2):331-350. Available from: https://eric.ed.gov/?id=EJ1368723
- Lee J, Seo YS, Faith MS, Barch F, Loja L. Do community schools work for high-needs students? evaluating integrated student support services and outcomes for equity. Educ Sci. 2025;15(8):1032. Available from: https://www.mdpi.com/2227-7102/15/8/1032